The Bio-Psycho-Social Model… ALL components are important!
Great guest blogpost by Ben Cormack about the components of the Bio-Psycho-Social model!
Ben Cormack runs Cor-Kinetic, an educational company that delivers continuing education courses in how to use movement therapeutically in a framework of modern evidence and science in pain, movement and rehabilitation. Cor-kinetic deliver courses worldwide having previously worked in the US, Europe, Australia and Japan. Here a link to his website: www.cor-kinetic.com
Cor-kinetic have provided educational services for the NHS, Elite level sports clubs and universities as well as individual physio’s, Osteopaths, Chiropractors, sports therapists, rehab, and personal trainers.
Ben has studied extensively in the fields of exercise and therapy.
Originally from a exercise background, Ben has gone on to study clinical sports therapy and widely in the fields of rehabilitation, pain science and movement over the last 15 years. Ben is also a keen blogger who occasionally gets some people reading them and hopefully enjoying them too.
His blog can be read HERE.
How many times have you heard “but the pendulum has swung too far!” in relation to the Bio-Psycho-Social (BPS) model?

Many people have voiced their concern that we are now forgetting the biological/biomechanical side, or the B in BPS, of things. Others have suggested that there is still way to much biological/mechanical thinking if you look at information on posture etc being presented to the public with regards to back pain or text neck.
IT ALL MATTERS!
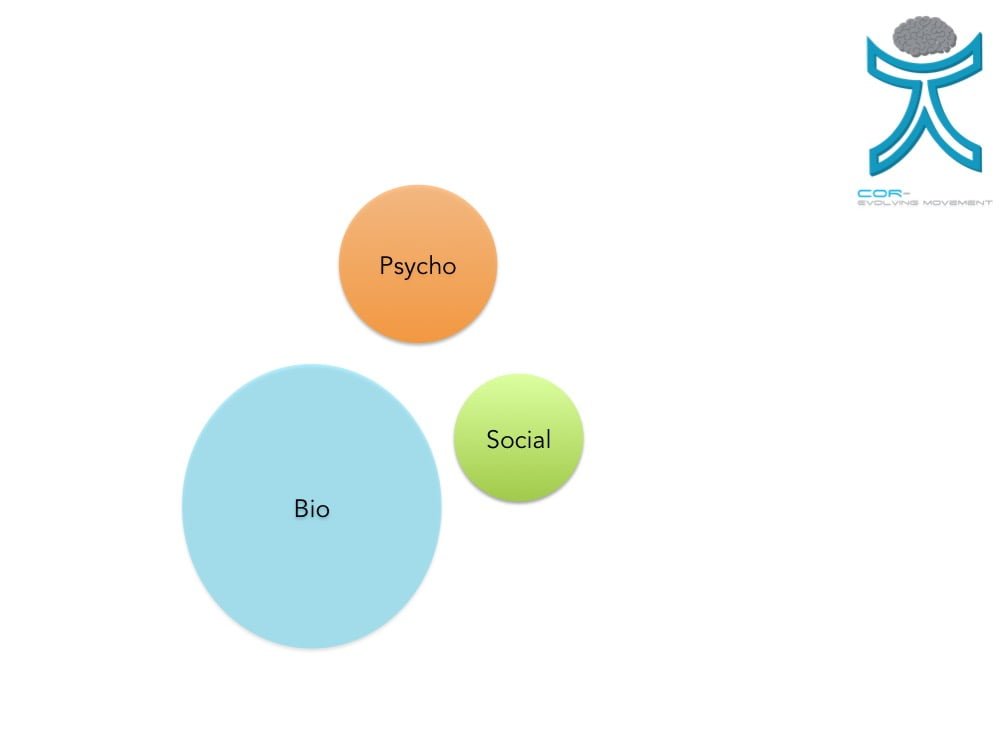
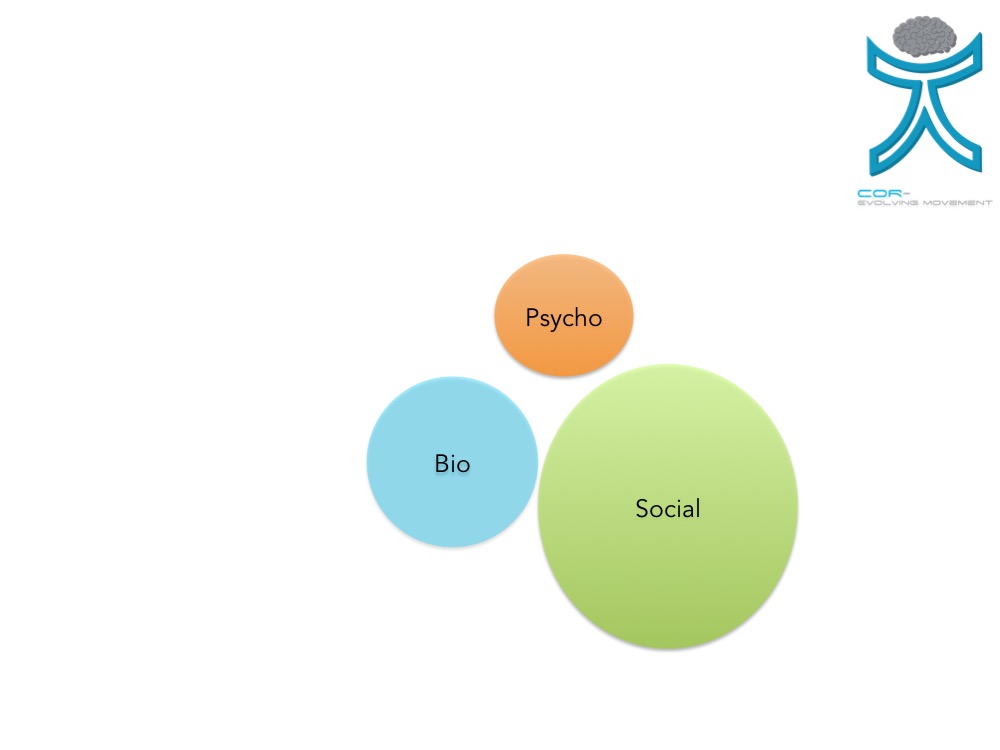
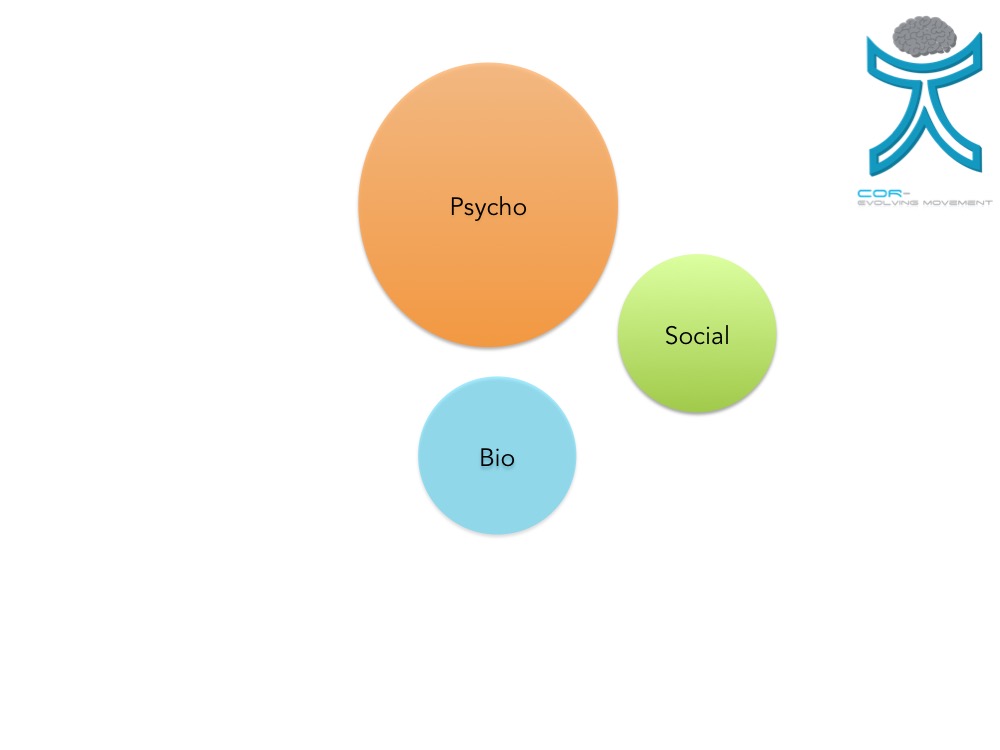
In reality ALL OF THE COMPONENTS of the BPS model matter when dealing with people, it’s just that different components may matter more or less for different people in relation to their current problem. One of the greatest tools in the therapist arsenal is having a REASONING process and this is being able to determine which component is MOST important to be managed first and how much of the available time and effort is put into managing it.
It is quite possible the same person may need an emphasis on different components at different times during the rehab process and that this reasoning does not remain static. Someone who is fear avoidant of a certain position or movement may need help that is targeted towards the negative perceived outcome of a movement, we could call this psychological, than the actual effect of the movement itself on the tissue, more biological. As the rehabilitation process progresses then biological and even biomechanical aspects may become much more important. You certainly can’t talk tolerance into a tissue, but you may have to talk to them first to get to the physical bit!
Unfortunately reasoning does not seem a particularly sexy subject for many; could it simply be too much effort? Roger Kerry wrote a great blog on this *Click Here* This is not the first time I have wrote about this either!
Human beings tend to like things put into neat little boxes or groups. This person is all bio, this one is all psycho, then we can bundle them off to the appropriate treatment or person to sort it out. Simples.
Oooor….. not so simple!
WHAT DO MODELS TEACH US??
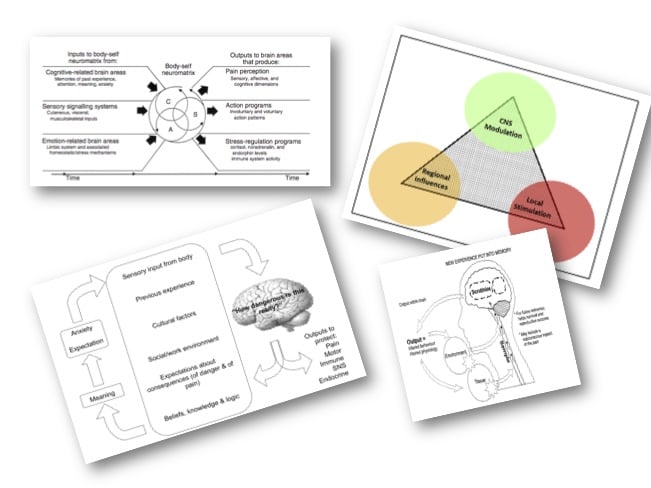
Modern models such as Melzack’s nueromatix theory of pain certainly DON’T provide us with answers but they DO help us understand that these things are not so simple and that there are always multiple contributors to someone’s current state rather than just a singular signal from the tissue. The famous George Box quote tells us “All models are wrong but some are useful” and my friend Todd Hargrove wrote a great blog on the subject *Click Here*.
USE THAT REASONING!
Perhaps the prevailing type of people that we see can cloud our reasoning? Our perceptions are influenced by our experiences, there is no way around this, and this could influence the overall weighting of importance that we place on the different elements of the BPS framework.
If you are involved mainly sports injury then you may see lots of acute muscle injuries that have a clear mechanism of injury and a well-defined recovery timeline. The biological aspect maybe the most prevalent and the major source of nociception is obviously, duh, the tissue and the damage that has occurred to it. For a therapist who deals with lots of postoperative patients, or the elderly, then simple increases in strength might work wonders.
If you are predominantly a therapist who sees runners then it might also be a similar scenario, you get a lot of runners who have simply run a bit too much, too soon and with a sharp spike in intensity. They may just need to manage their running program, and load to their tissues, a bit better and everything will be hunky dory! Although tissue-healing times might be a useful piece of information, why would they need hours of pain education on ion channels etc (not to say this is always the case)?
It could be however that a runner with an exercise compulsion, weight or stress management issues or heavy social involvement with exercise struggles to manage their load not through a lack of education but because of issues more weighted to the psychosocial factors. This may place much more of an emphasis on the psychological or social components of the BPS model that maybe contributing to someone’s pain.
If you work in a chronic pain clinic then you may spend a shit load of time talking about pain and it may influence your patients greatly, how much they can lift or spikes in their training program might not be of primary concern. Someone who works in the National Health Service in a traditionally poor area with people who are unemployed and depressed and under lots of social pressures might place a greater emphasis on stresses that these kind of situations put people under, and how they maybe able to help people manage some of them might form a greater part of the assessment and treatment process. Low socioeconomic status may affect general health, access to exercise facilities or the time someone can actually spend exercising so these factors may impact on the actual ability to do the bio part.
A 10 year history of lower back pain might also display a different weighting of the BPS components. If we use the evidence base this maybe much less about tissue tolerances and spinal curves and much more about someone’s perception of their capabilities, movement behaviours and expanding their levels of self-efficacy with regards to physical activity. However the involvement of an exercise program, the bio, may work wonders for their back pain, we just don’t know exactly WHY yet.
The ability to reason is a really great tool, and one that is potentially underused. The ability to apply this reasoning to the person standing in front of us IS hard and potentially brain intensive but is also likely to give us the best results.
SUMMING UP
- Everything matters
- Just in different proportions
- This may change over time even in the same person
- Models tell us things are complex and multifactorial
- They don’t give us answers
- Our situations bias our views
- Reasoning is the best tool we have
You can watch more of Ben Cormack on Trust me-ED. You can sign up and watch all lectures 7 days for free.
He did one webinar about low back pain and exercise:
And one about a modern approach to movement and exercise:


