Pain, identity, motivation, control and choice ; A framework for change
Connor is a physiotherapist and strength and conditioning coach from Newcastle, Australia. He works on public health research; his focus is on knowledge implementation and capacity building for GPs in low back pain and primary prevention, and in understanding the pain burden in children. He also works clinically in a youth athletic development facility and as strength and conditioning coach for a semi-professional rugby league team. He is passionate about improving the delivery of healthcare for all stakeholders.
Follow Connor for evidence-based information about pain, research and strength and conditioning on Facebook here or Instagram here. Or read more of his blogs here.
Pain, identity, motivation, control and choice; a framework for change


Pain and identity
Pain that has been around for some time is no longer simple. It becomes interwoven into the beautiful tapestry that is life, which makes it hard to define and identify, but also really hard to accept and move on.
This doesn't mean it can't change (see title of series), it simply means we may need to accept our identity the way it currently is. It's kind of like saying, 'OK, well that happened, so now what?' Acceptance is the first step to creating change.
This is based on Acceptance and Commitment Therapy, which it has to be said does not show any greater effect than control groups in a meta-analysis by Hughes et al 2017 in reducing pain intensity and quality of life (Ref, Ref). But, this is potentially not what we are after when talking about creating a framework for change - do we want to abolish pain or do we want to create a pathway for a new normal?
It may become part of the 'ego' or identity; the astute clinician will become very aware of this and be sensitive to this issue. But an important next step is to appreciate just how much this impacts on daily life and how much meaning is ascribed to this pain? People attend for treatment, not because of their pain, but because of the suffering it engenders - they are having trouble being themselves, they are having trouble taking part in the things they want, need or love to do. We are here to change their lives; to help them regain these beloved and meaningful activities.
And so, in the clinical environment, it is always very useful to first consider how your patient is motivated and how their pain impacts upon their motivation.



Pain and motivation
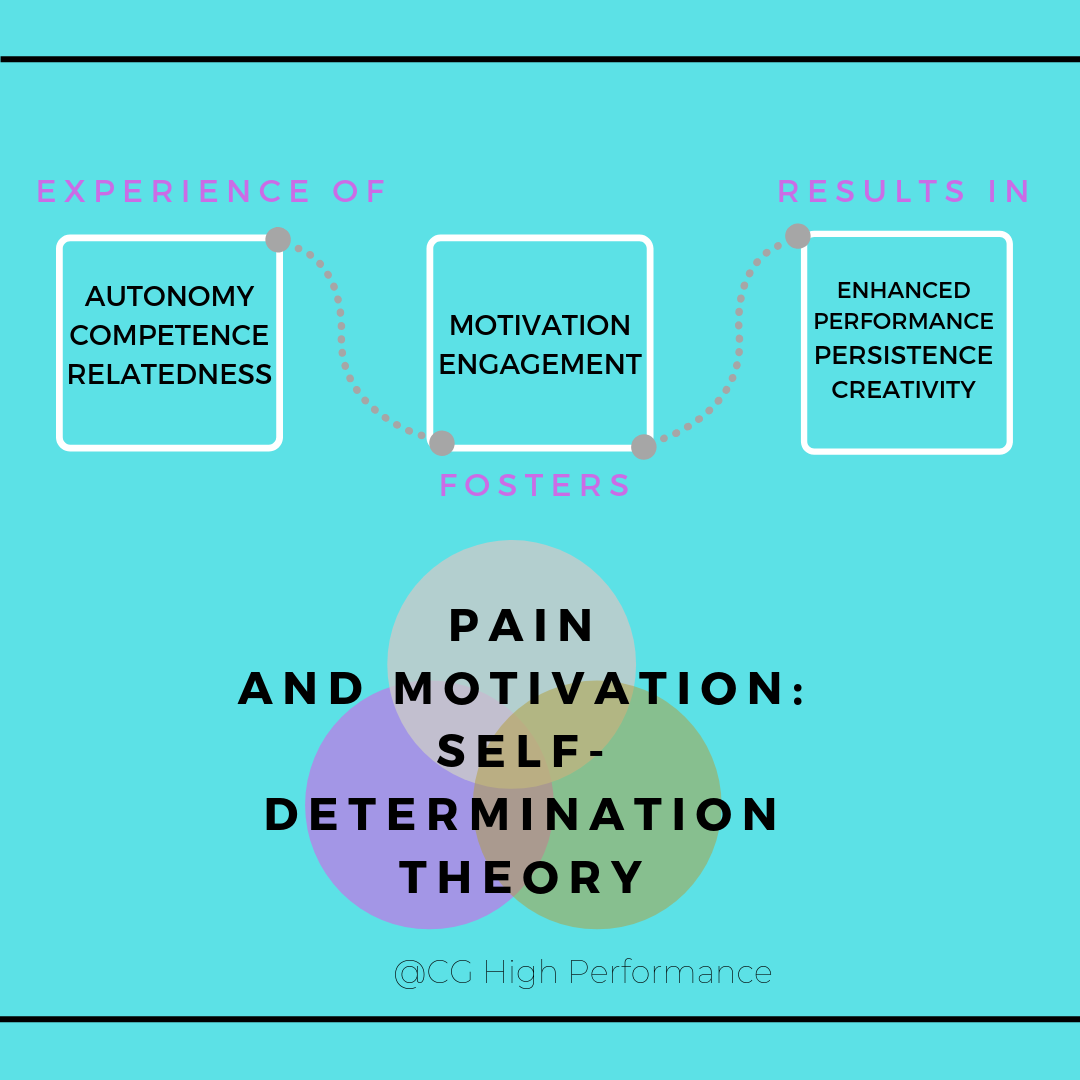
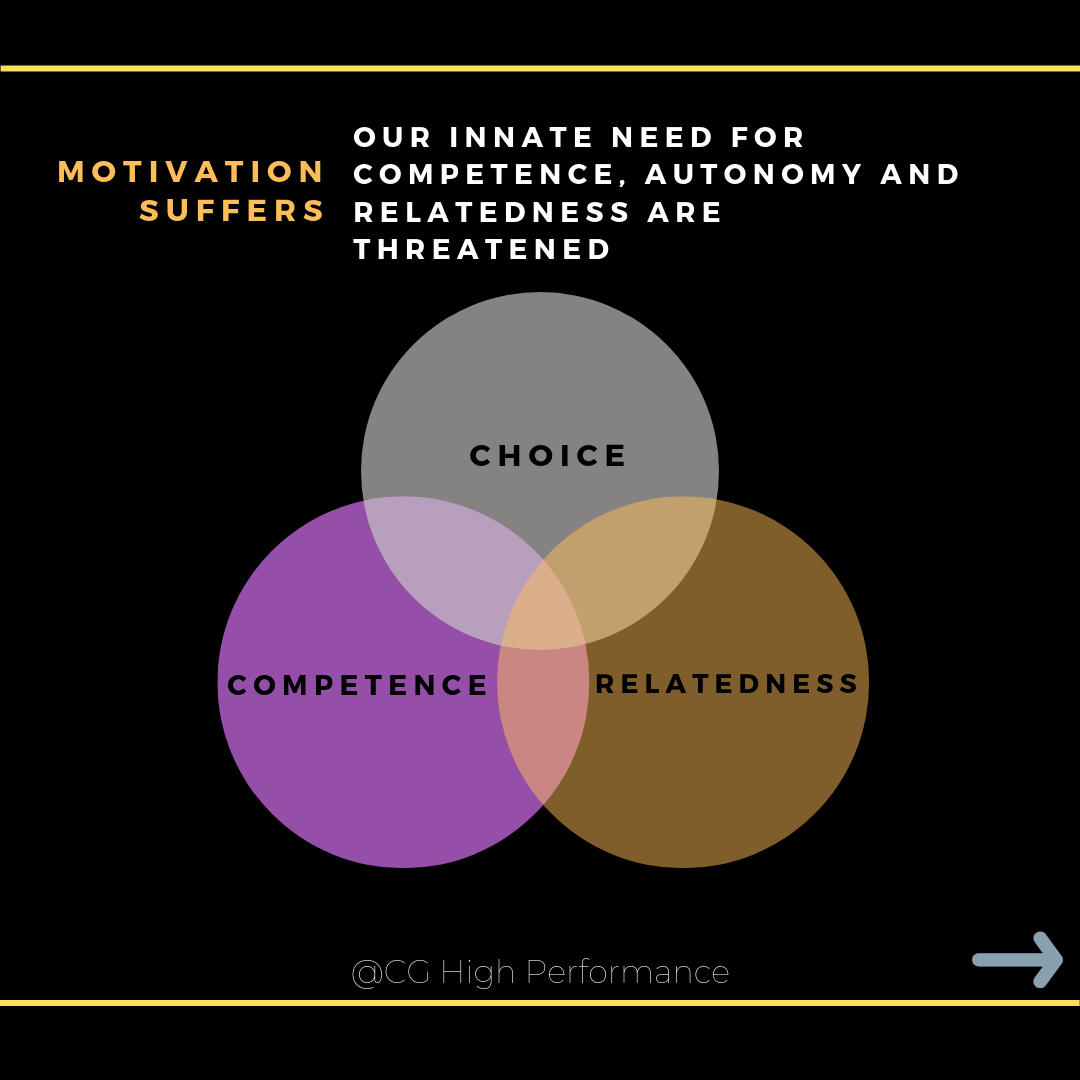
Self-Determination Theory (SDT) states the quality of motivation is enhanced when any of these needs are satisfied and optimized if all three are satisfied.
Autonomy involves feelings of willingness and choice in regards to activities undertaken; relatedness refers to feelings of closeness to other people; and competence involves feeling able to master challenges and having effective interactions with the environment.
First we build competence, then we can instill autonomy and last, relatedness is something we can encourage. Self-selecting practice variables has been shown to improve motivation in a review of motor learning and medical training literature by Sanli et al 2013 (Ref). The caveat is that this has had limited testing in painful populations.
The huge implications for social contexts in motivational theory is an untapped well, but has some good theoretical work in painful populations (Ref).



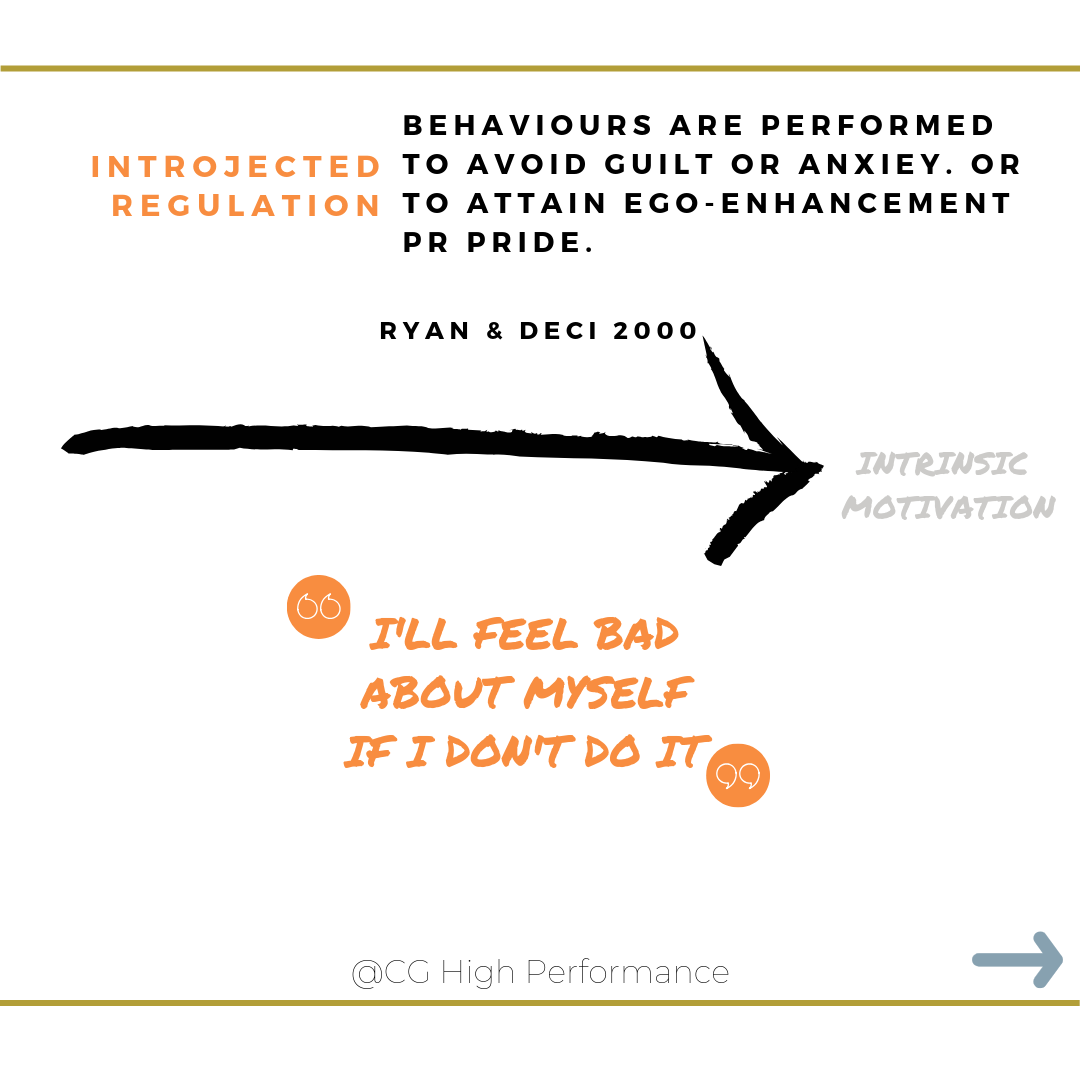
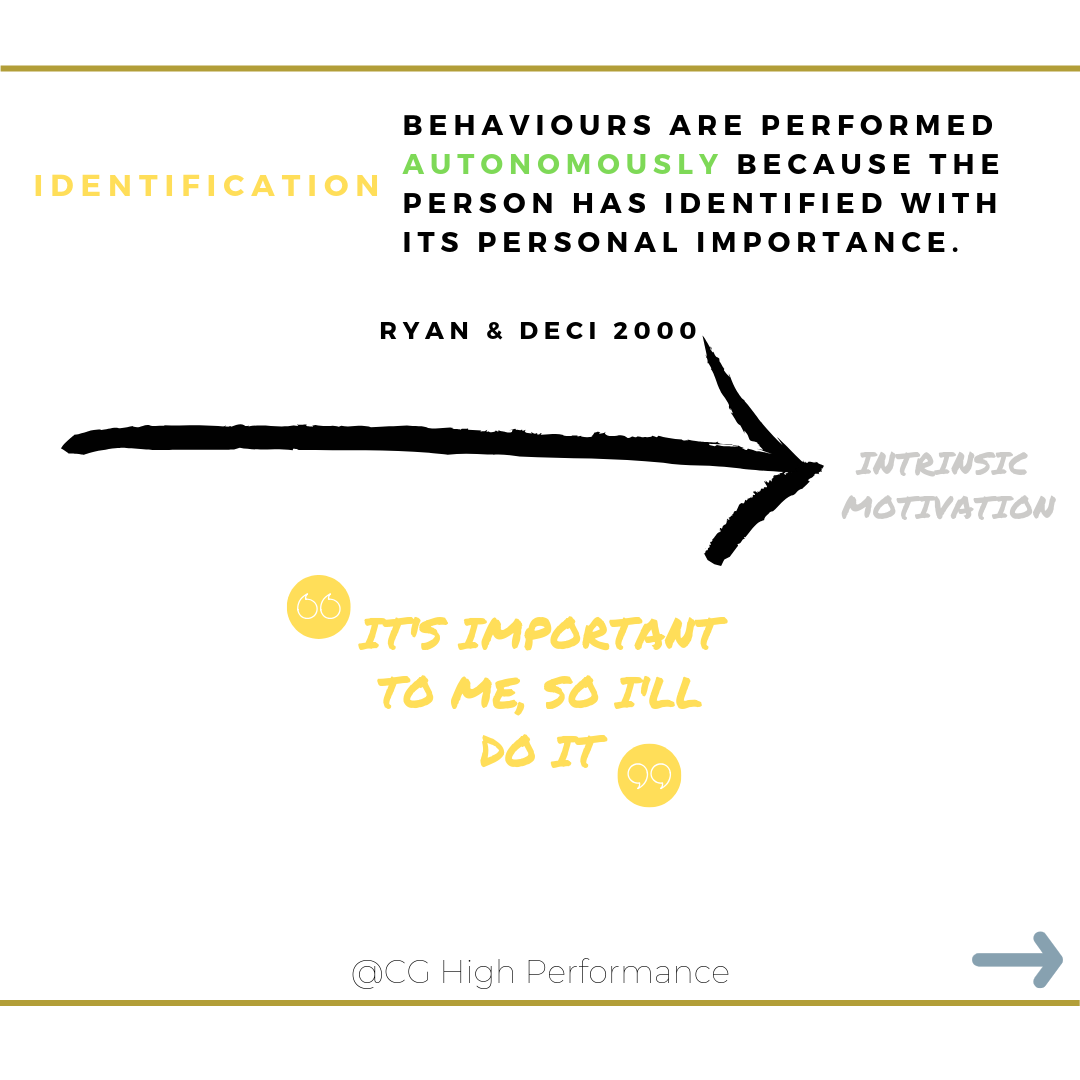
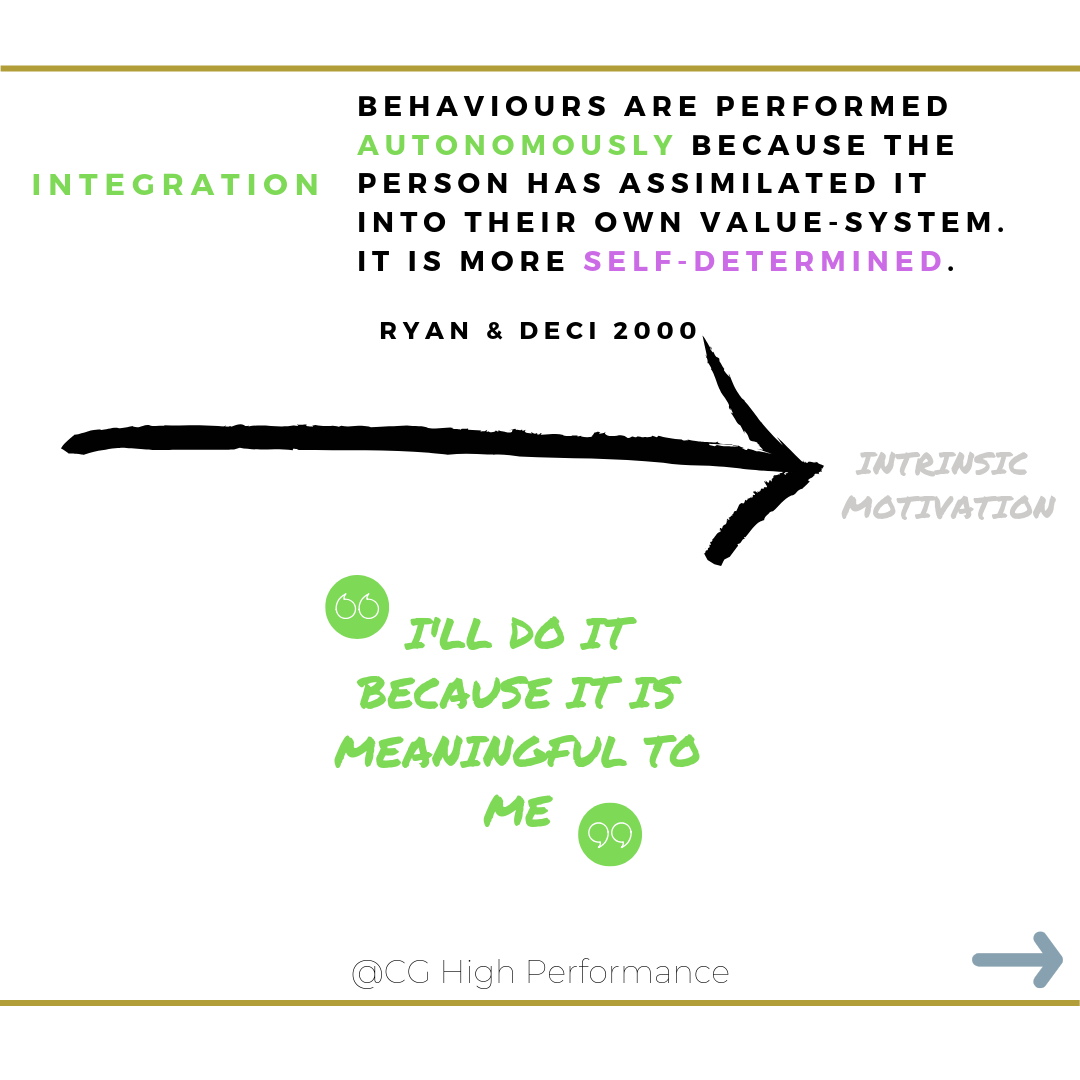
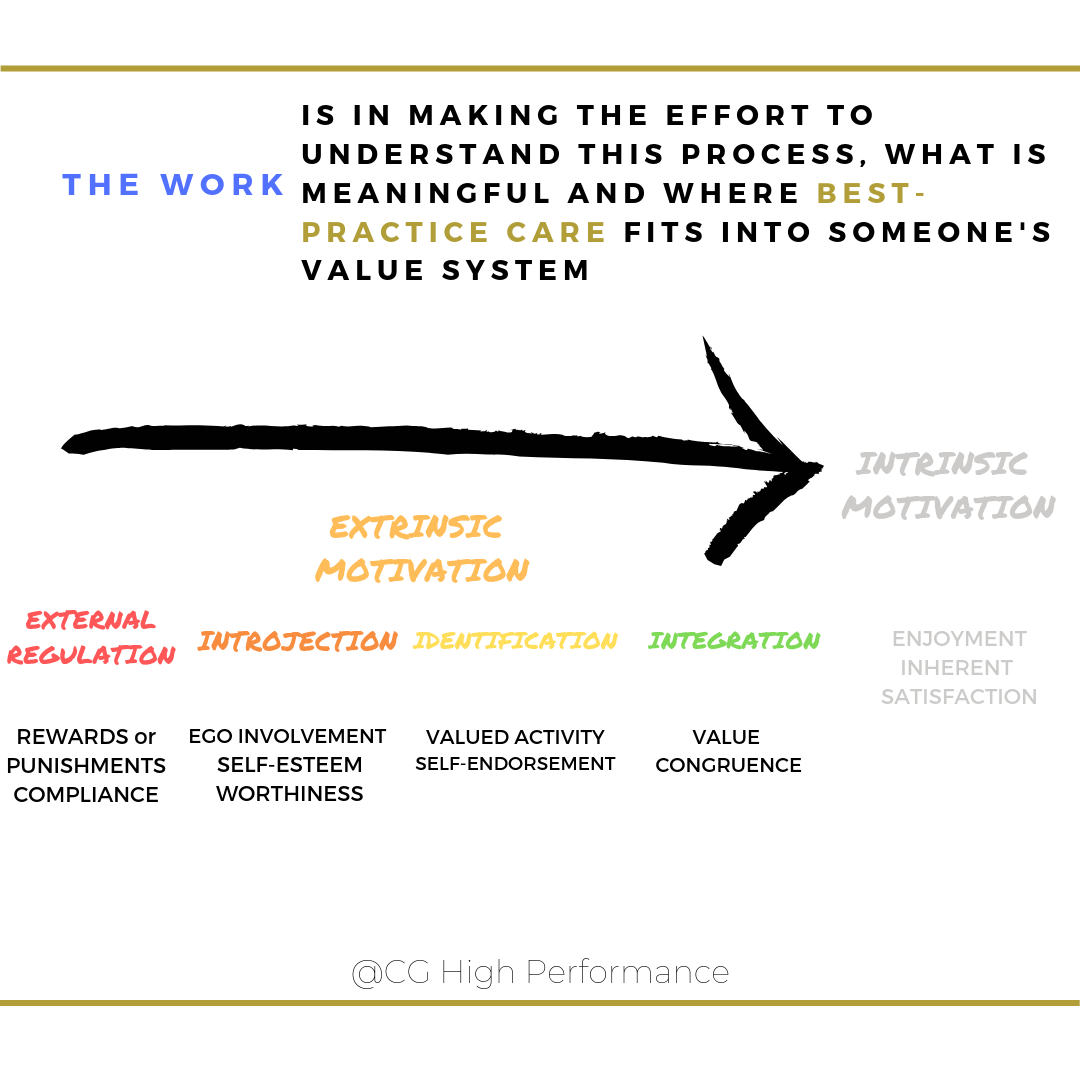
Extrinsic, intrinsic and the regulation of motivation
If we understand some basic theory about how motivation is constructed within individuals, we can delve further into the intricacies.
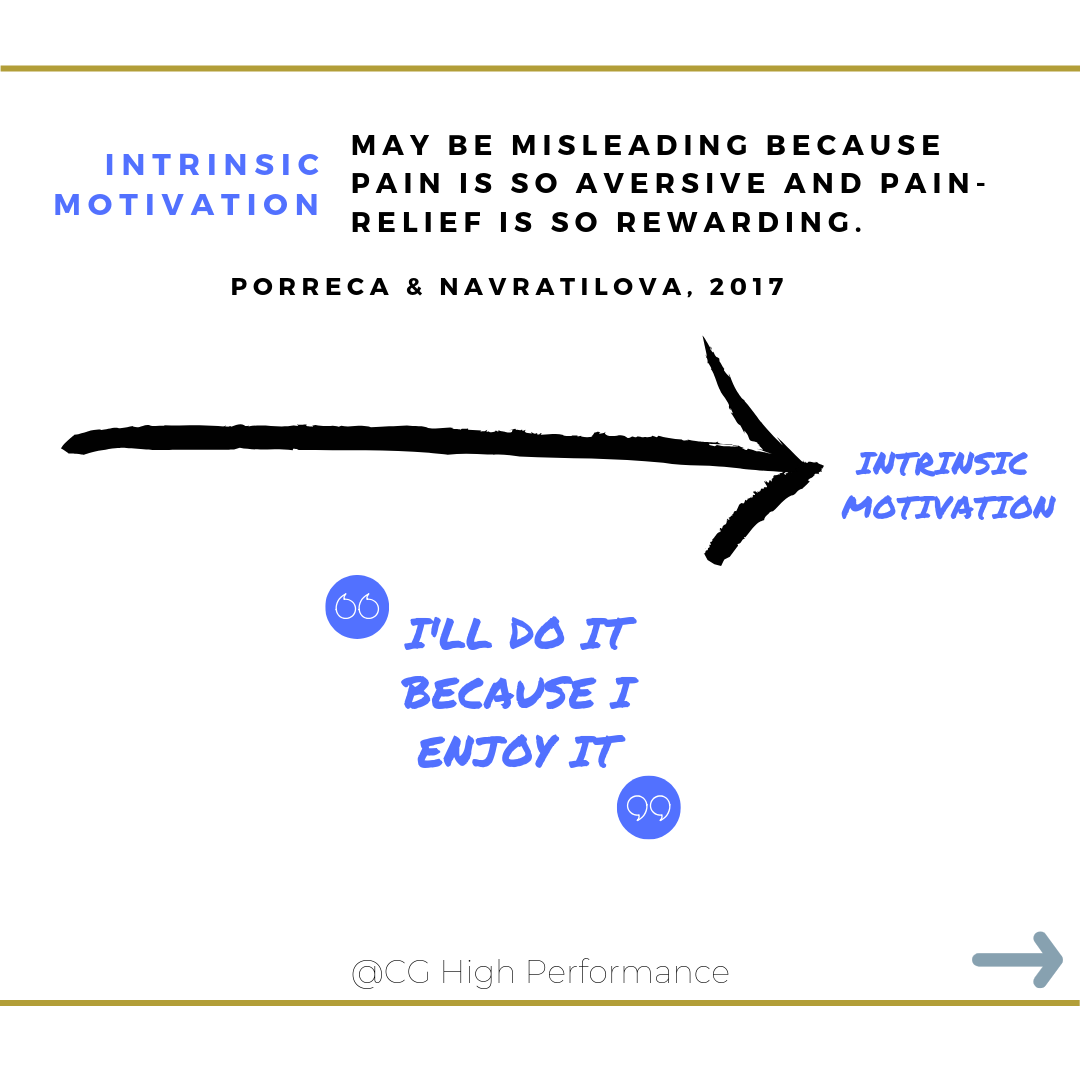
In humans, intrinsic motivation is not the only form of motivation, or even of volitional activity, but it is a pervasive and important one. It has been lauded due to its ability to encourage creativity and curiosity driven behaviours. That funnily enough, aren’t necessarily adaptive or integral to an organism’s survival.
Intrinsic motivation in pain and health has not really been studied much, but the relationship between the two variables is likely much more complex than we would initially think. But we do know that the brain circuits mediating the reward of pain relief and relief-induced motivation are significantly impacted as pain becomes chronic. How much is the relief of pain a driver in what people do?
Do we need to take intrinsic motivation off the pedestal when it comes to pain management? Do we instead need to focus on the regulation of motivation in people - that is how they process and integrate behaviours that are beneficial in pain?
Taking the time, effort and care to ensure that people can understand the importance of treatments to them and how it relates to their value system is something every clinician should strive for.
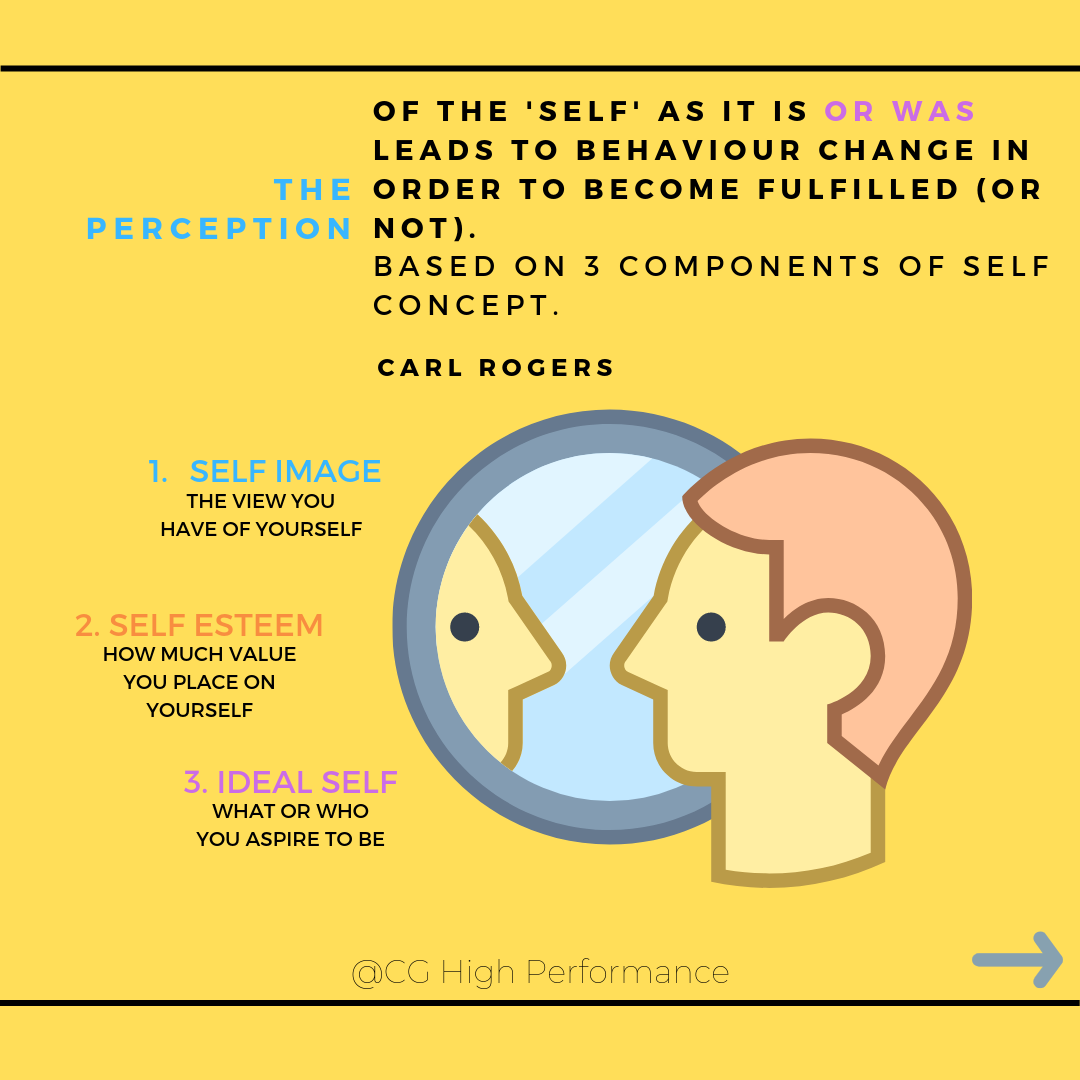

Pain and concept of the self
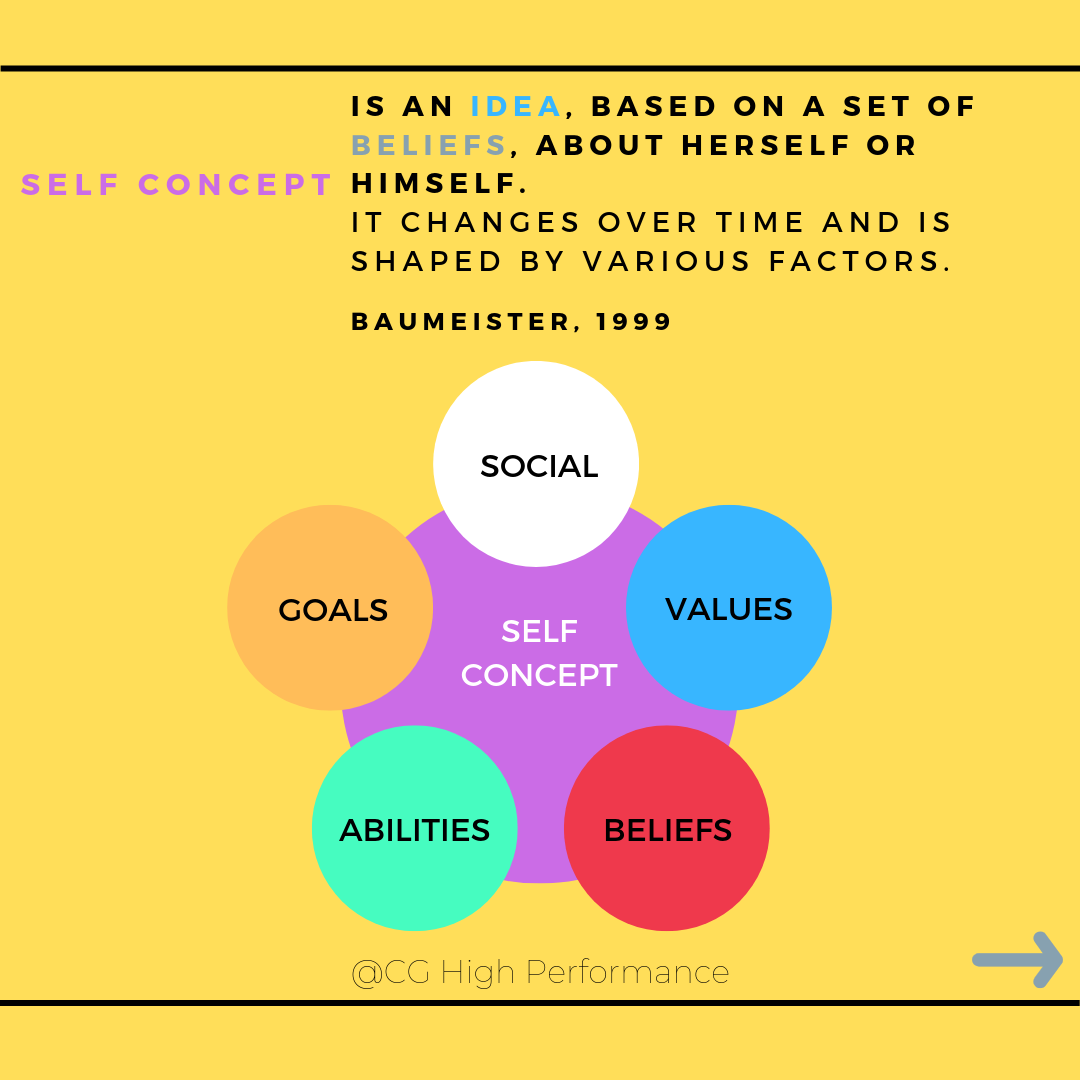
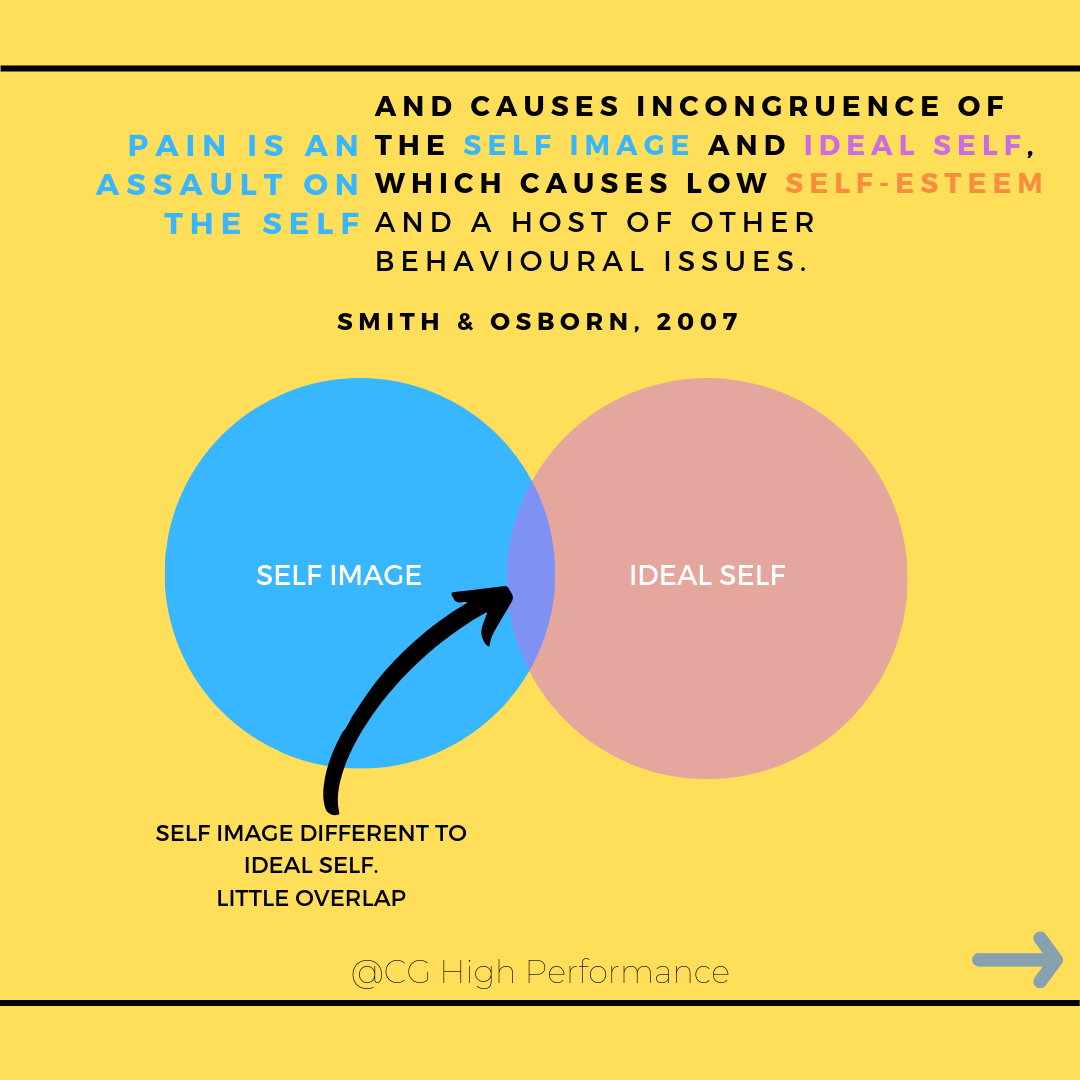
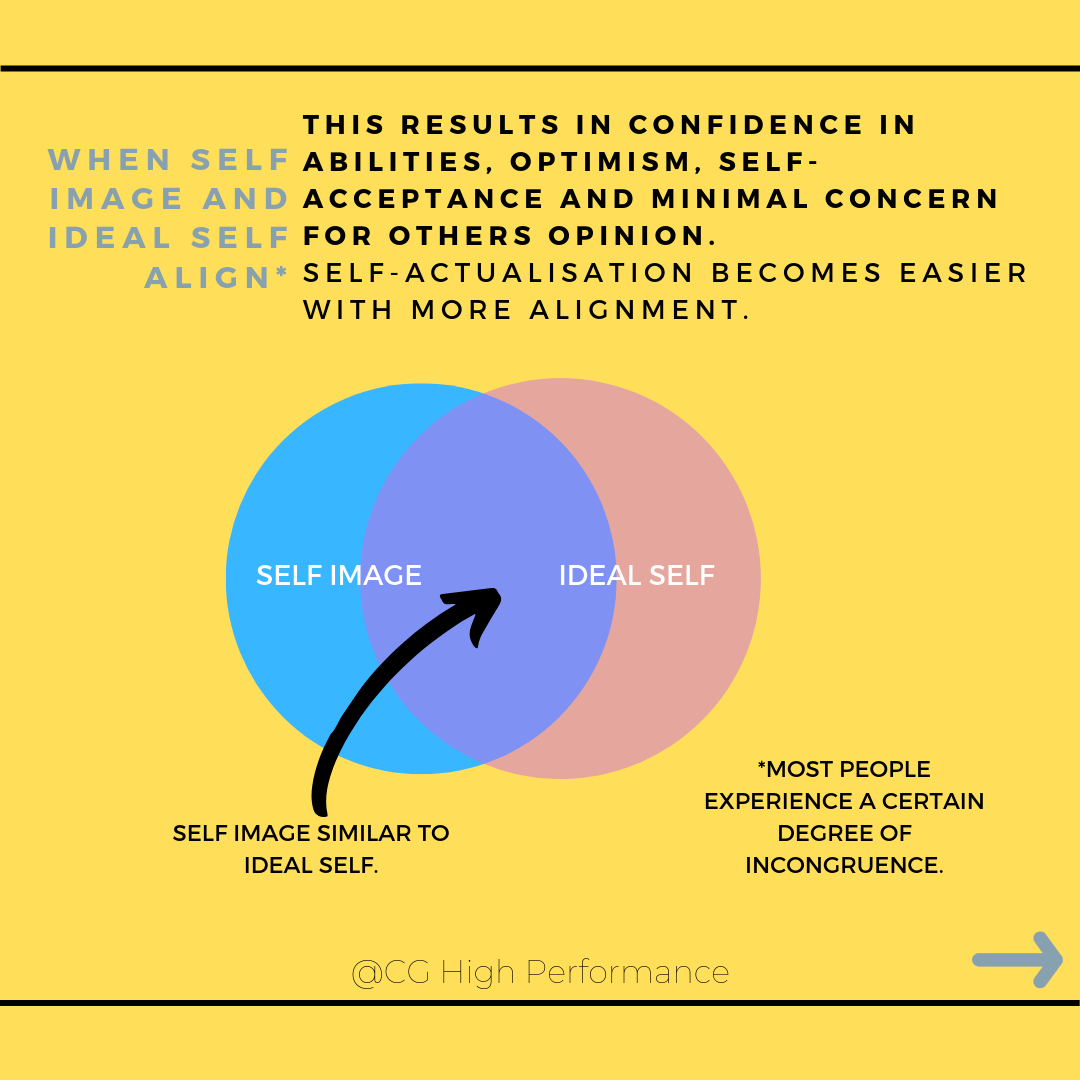
Pain can have a profound impact on the sense of self. The self concept is an idea about oneself, based on a particular set of beliefs. Pain can cause a mismatch between self image and the ideal self, which can cause tension, confusion and other maladaptive behaviours.
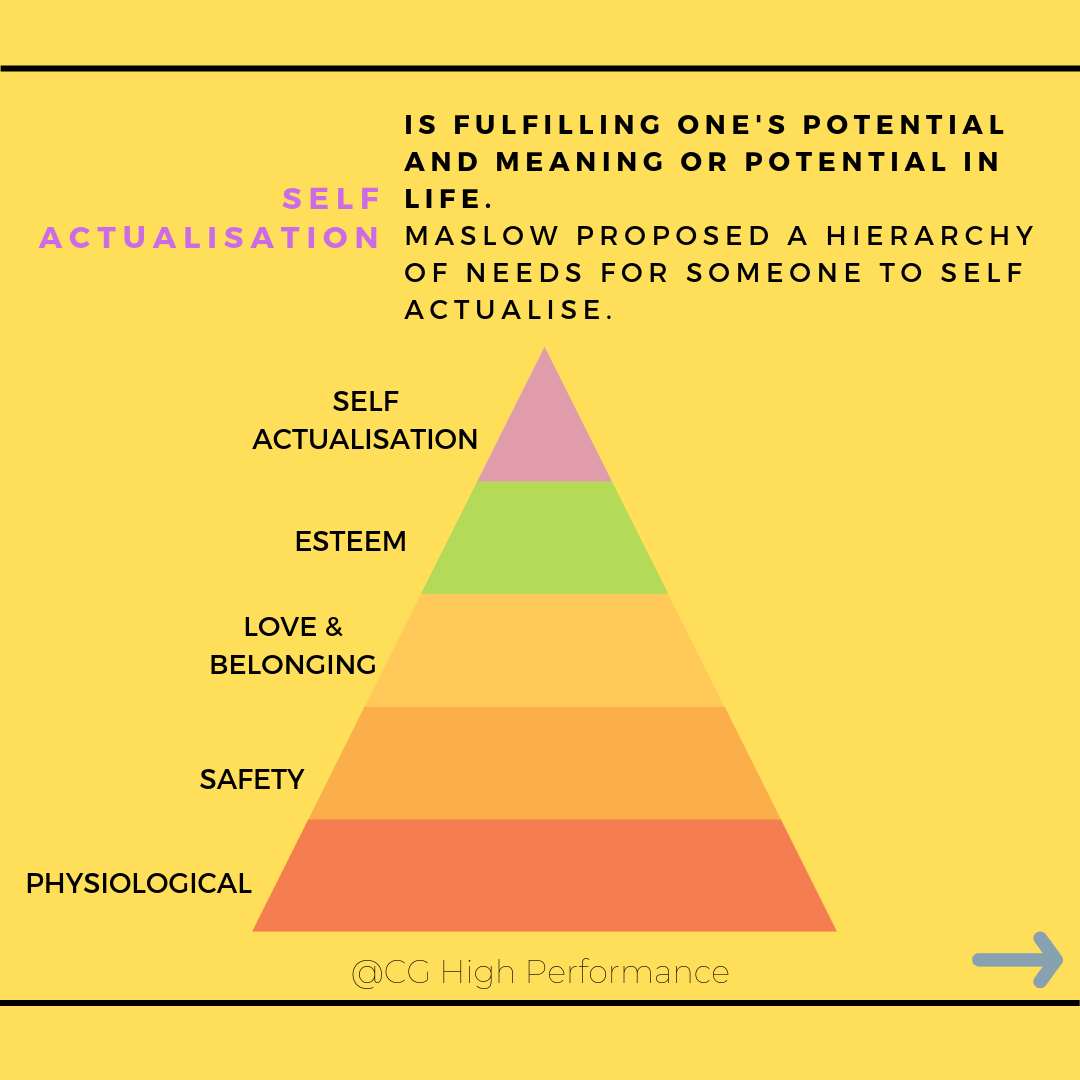
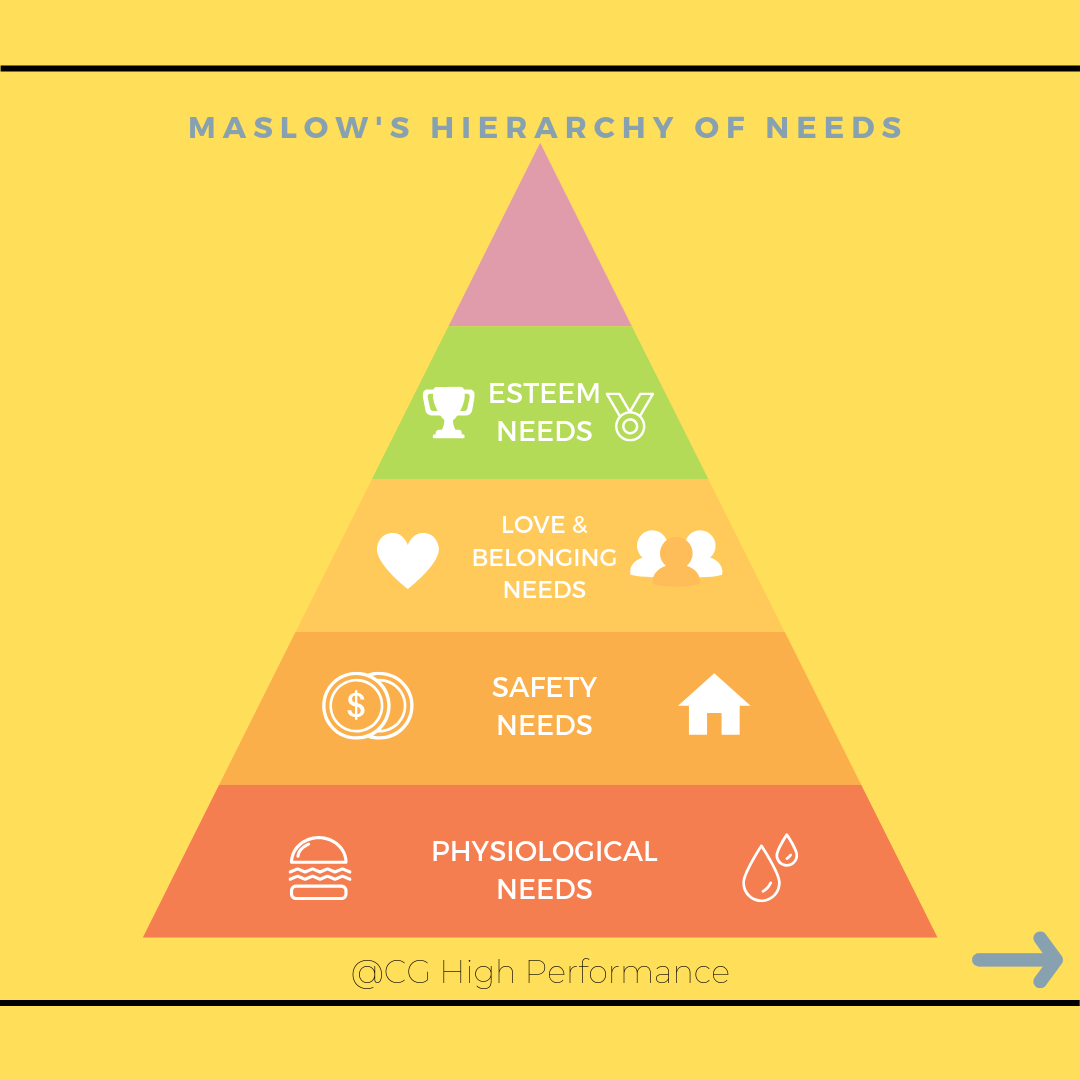
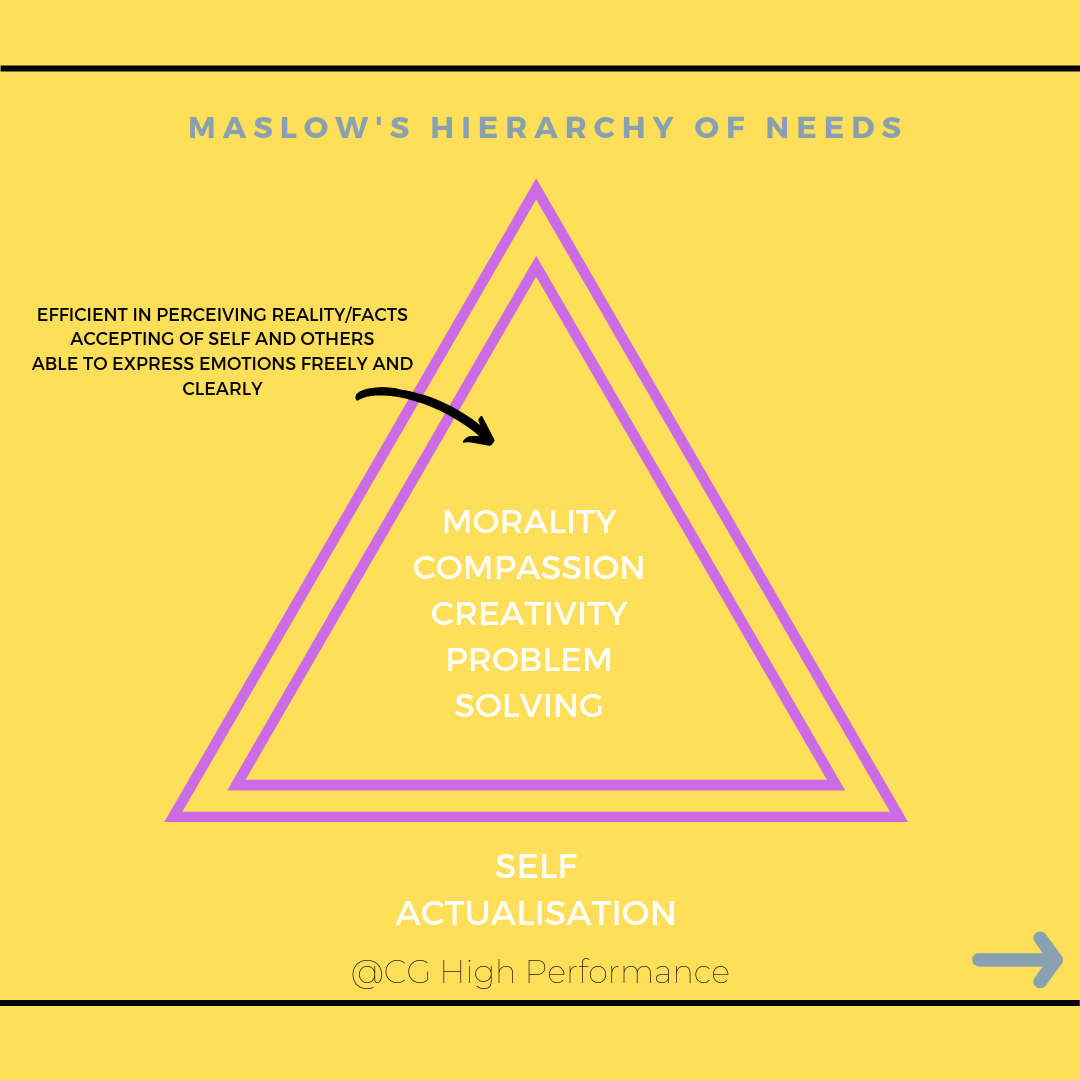
When there is a close alignment of the self image and ideal self, it makes self-actualisation more likely. Self actualisation is a concept proposed by Abraham Maslow and he proposed that every individual is consistently aiming for an ideal self, to self-actualise. Every person is capable of moving up the hierarchy, but there will be inevitable fluctuations and movement may not always be a simple linear progression. Some people may have lives, in which higher levels are met, but may be prevented from meeting lower-level needs. These are:
1. Basic physiological needs like food, water, sleep.
2. Security needs like employment, a roof over your head, or even physical health.
3. Love and belonging needs like family or a social group.
4. Esteem needs like individual achievement, recognition by your peers.
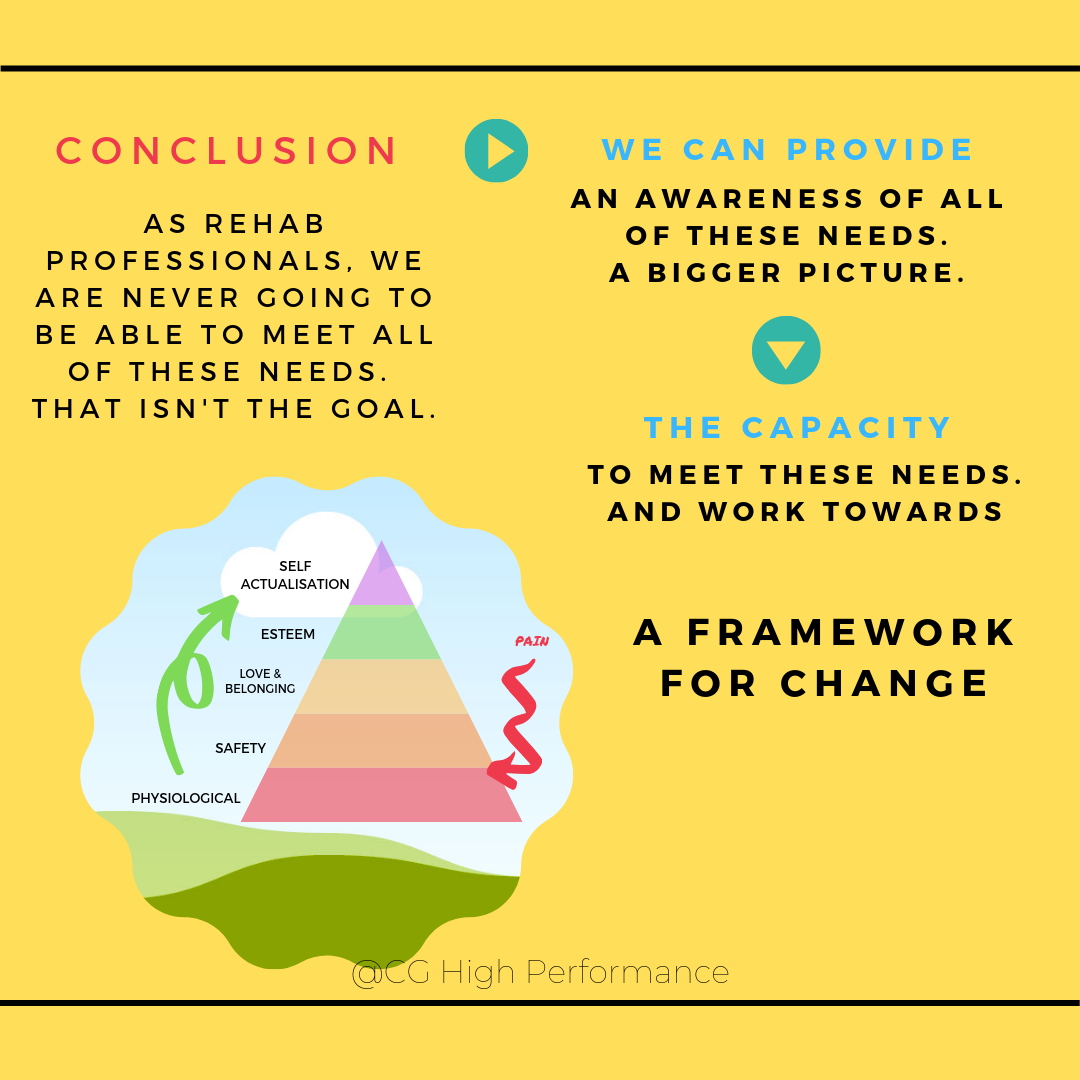
In managing people in pain, we also need to understand some basic theory about what drives the individual in front of us, their needs. Likely there are gaps in these needs - we shouldn’t just be proficient at realising the physical issues or needs!
In helping the patient create a framework for change, our job is to create awareness, where there may be none, on the bigger picture. Of where they have neglected some other really basic needs that they may have, or to instil a good common-sense thinking to consider what the ‘ideal self’ may look like in the face of adversity or with significant barriers.
The astute clinician builds capacity (rather than breaks it down) and helps provide the tools to meet these needs.
Pain and control
Healthcare is an inherently disempowering environment. Human behaviour is, for the most part, irrational and based on our perception of reality.
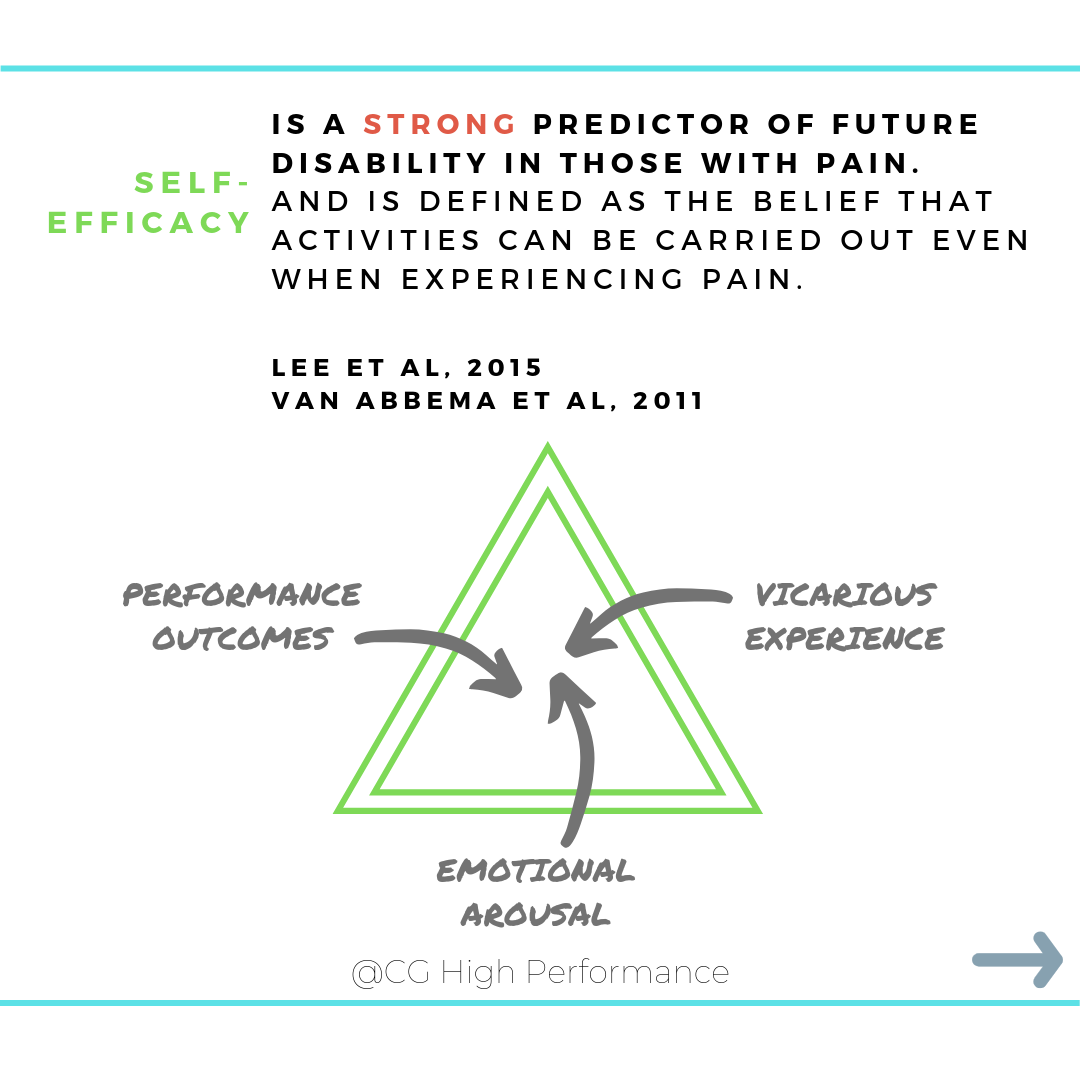
In the land of pain and disability, self-efficacy is king. It is one of the strongest predictors for future disability for those in pain. It is composed of different aspects, like previous negative or positive experiences in performing a task, watching other people’s performance (vicarious experience) and the sensations people get from their body in performing tasks (emotional arousal). It is strongly influenced by verbal persuasion, you can encourage or discourage self-efficacy just with your words and it equates to the belief that someone can do something.
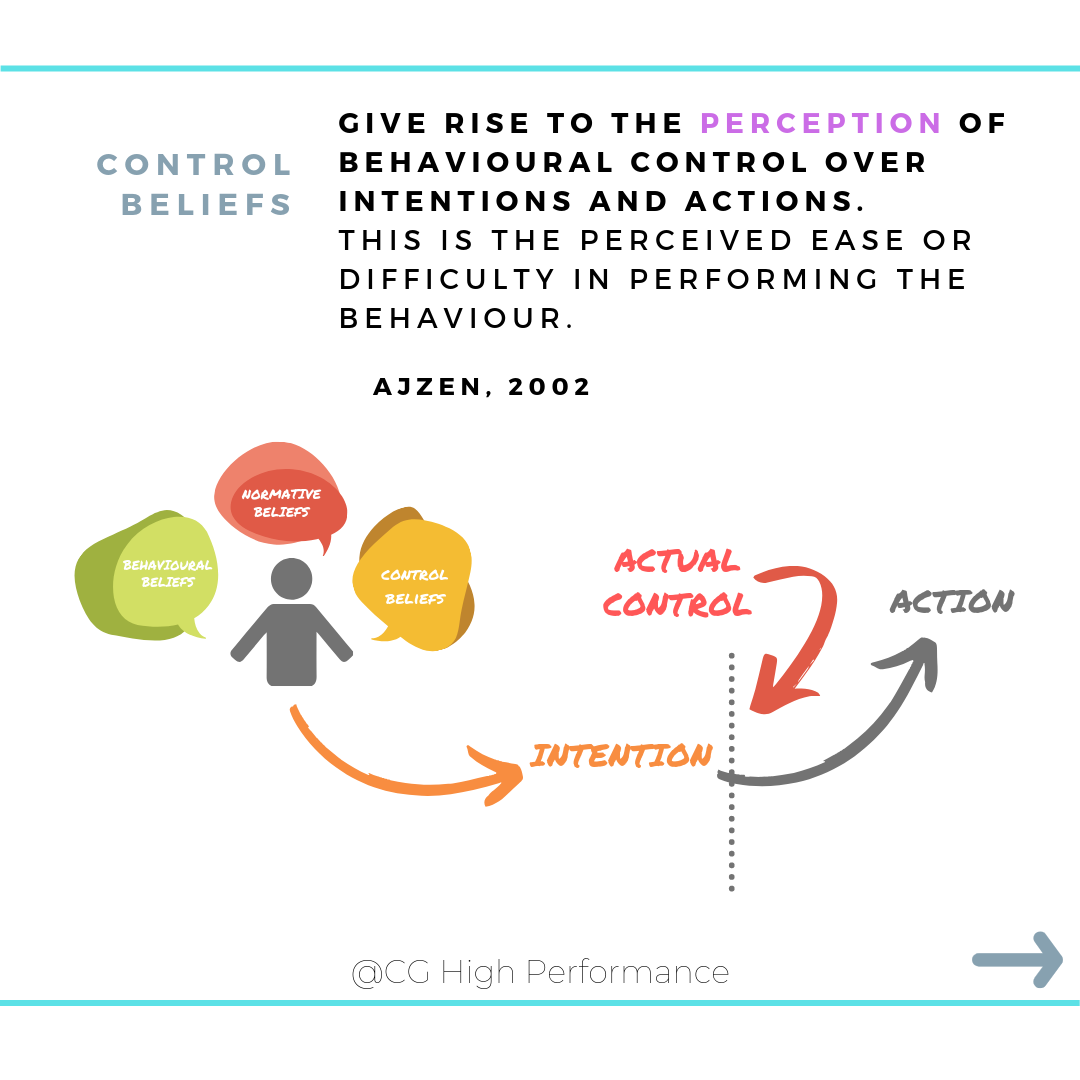
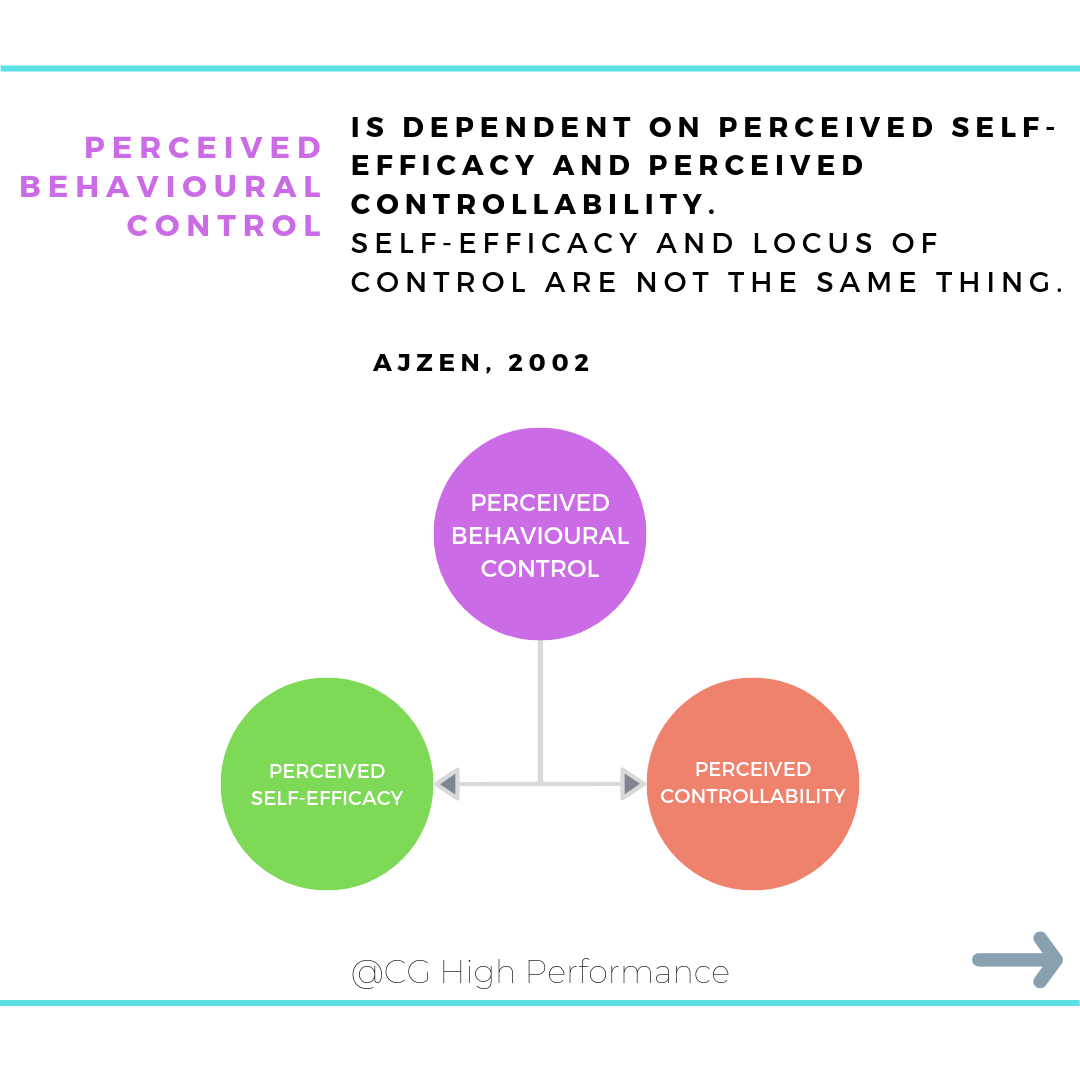
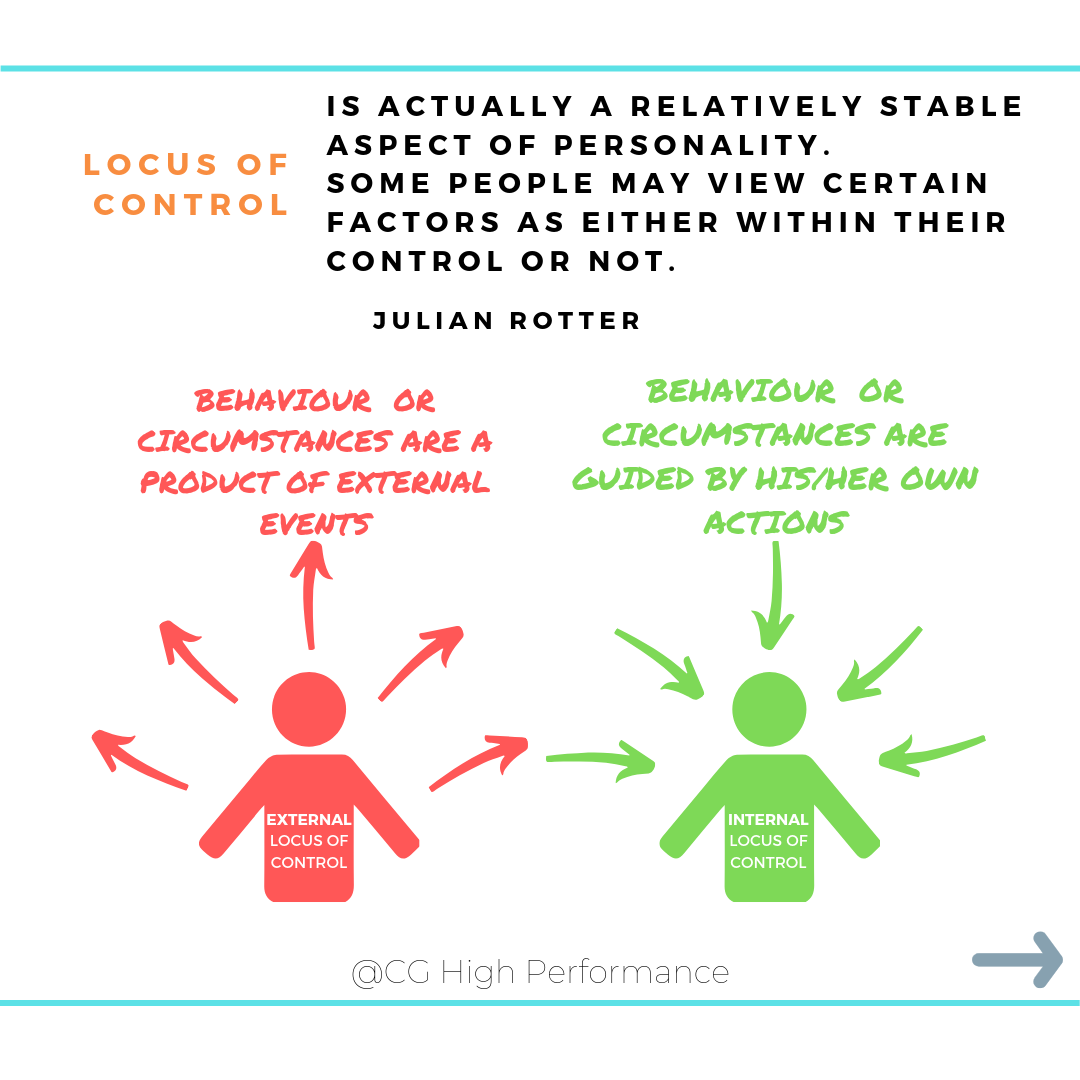
A different, but related, concept altogether is locus of control. It is generally a stable aspect of personality and is the degree to which people believe they have control over the outcome of events in their lives. There is a lot of work done in general healthy behaviour and locus of control, but not a lot in painful conditions. So we don’t know a lot. But it has been shown that people in treatment experience greater external control beliefs compared to wait list controls by Keedy et al (2014).
But perspective is important. It is our job to delve deeply and alter or correct if our patient’s beliefs about what is and isn’t within their control, and when it comes down to it this might be a lot more than they think!
So understand that self-efficacy is incredibly important and you need to have an appreciation of how internally or externally controlled your patient is.
Pain and choice
To conclude, as a clinician, you have a choice; to learn these things about your patient. To understand it isn't as easy as, 'If we do x, I will see y outcome.' You have a choice to delve deeply into the complex world of identity, motivation, and behaviour.
Our patients all have choices as well. We can provide the awareness and offer a better, more adaptive solution. Whether this is physical - or in the line of these posts - more behaviourally.
What's your choice?
Ref:
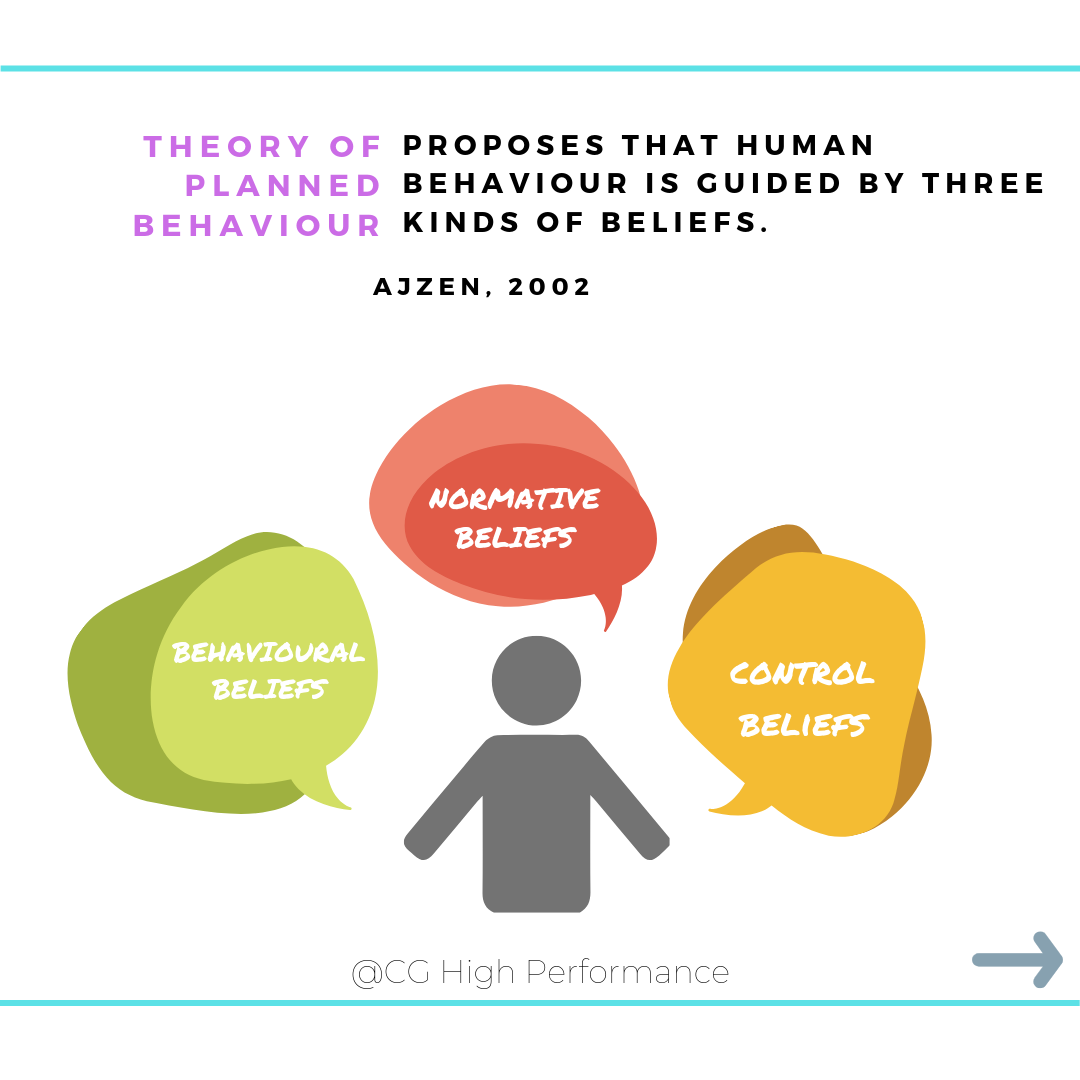
Azjen, 2002 https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1559-1816.2002.tb00236.x
Baumeister (1999) https://psycnet.apa.org/record/1998-06436-012
Chiviacowsky et al 2012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3487418/
Chiviacowsky & Wulf 2005 https://doi.org/10.1080/02701367.2005.10599260
Lee et al 2015 (great meta-analysis) https://www.ncbi.nlm.nih.gov/pubmed/25760473
Keedy et al 2014 https://www.ncbi.nlm.nih.gov/pubmed/25328476
Porreca and Navratilova (2017) Reward, motivation and emotion of pain its relief https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5350036/
Ryan & Deci (2000) Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions http://selfdeterminationtheory.org/SDT/documents/2000_RyanDeci_IntExtDefs.pdf
Sanli et al 2013 https://www.researchgate.net/publication/235691534_Understanding_Self-Controlled_Motor_Learning_Protocols_through_the_Self-Determination_Theory
Smith & Olsen (2007) https://www.tandfonline.com/doi/full/10.1080/14768320600941756
Van Abbema et al 2011 https://www.ncbi.nlm.nih.gov/pubmed/21516301


